
When Sara Schultheis was in third grade, she suddenly dreaded going to the school cafeteria. The typically extroverted, hard-working student became scared of public places, lost weight and avoided favorite activities.
“It didn’t make sense,” said mom Shannon Schultheis. Shannon and her husband Todd couldn’t figure out their daughter’s sudden behavior change. She previously enjoyed and excelled in school.
Sara’s teacher, school nurse and school counselor recognized the abrupt changes in Sara’s once-happy demeanor and urged her parents to seek help.
“If I don't help her, it’s neglectful,” said Schultheis of her realization that intervention was necessary. “I have to help her, the same way I’d help her if she had a cold.”
Sara was diagnosed with an anxiety disorder. While anxiety or depression may sound like grown-up problems, Sara is proof that mental health conditions do impact children and youth and don’t discriminate based on zip code or socio-economic status. They’re not reserved for children who’ve experienced a significant traumatic event. In Sara’s case, the internal pressure of receiving her first letter grades may have been a trigger for the student, whose personality tends toward perfectionism. And mental health conditions are much more common than parents realize. As many as one in five children and youth have a mental health condition, according to the National Institute of Mental Health. That’s four students in an average Oklahoma elementary school classroom.
Sara was placed on a small dose of anti-anxiety medication to help calm her brain and body’s physiological fear responses. With the help of a counselor, she learned to manage her behavior. 
Sara’s support team at school communicated regularly with her parents, who were grateful they didn’t normalize or dismiss Sara’s behavior, but rather embraced her for who she was in a difficult time. After a year, Sara was able to quit taking the medication. She’s now a well-adjusted high school senior and her parents credit early intervention for helping her accept and overcome the challenges of anxiety.
As the director of Oklahoma City private school Warm World for the past 15 years, Shannon Schultheis occasionally and empathetically helps other parents walk a similar journey. Half of all mental health conditions begin by age 14, and even among the school’s preschool through kindergarten population, symptoms surface as young brains develop. The National Survey of Children’s Health reports 26 percent of Oklahoma children age 4 months to 5 years are at moderate to high risk of developmental or behavioral problems.
“When I started, the incidents were few and far between,” said Schultheis. “Now every year we have multiple children whose needs vary off the typical developmental path.”
Though Schultheis has been on the receiving end of a similar conversation, talking with parents about developmental and mental health concerns doesn’t get easier. But she and her teachers value their partnerships with parents, and though they aren’t diagnosticians, they are well-versed in what typical development looks like.
“Part of our ministry to parents is to share feedback,” said Schultheis. “If we don’t have those conversations with parents, no one is. And then there’s no opportunity for early intervention.”
 The Epidemic
The Epidemic
According to the Oklahoma Department of Mental Health and Substance Abuse Services (ODMHSA), Oklahoma has some of the highest rates for mental illness, ranking third in the country. In fiscal year 2015, between 700,000 and 950,000 adult Oklahomans needed services like those provided by ODMHSA. Less than 200,000 received them. The state’s most recent budget failure equates to another $2.1 million in lost funding for the department, which means fewer Oklahomans receiving critical treatment.
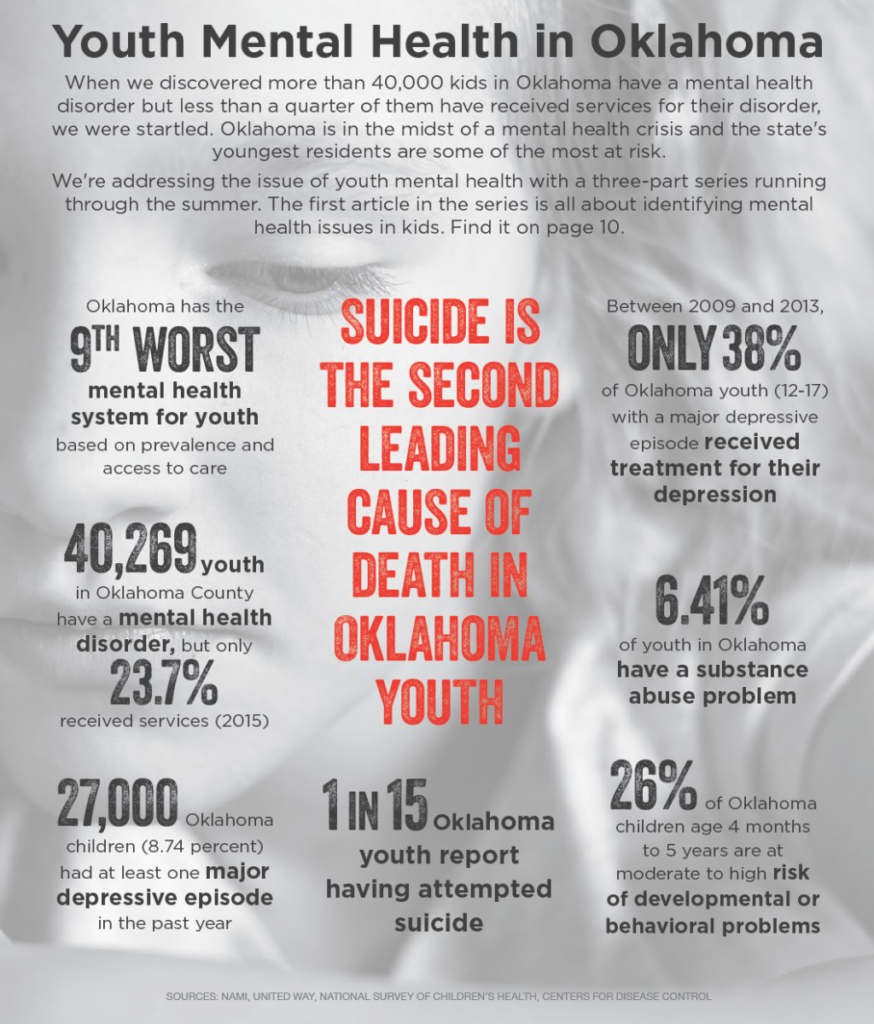
The lack of support for mental health impacts children, too. In 2015 more than 40,000 youth in Oklahoma County alone had a mental health condition, but not even a fourth of them received services. Almost nine percent of Oklahoma children had at least one major depressive episode in the past year, but between 2009 and 2013, only 38 percent of Oklahoma youth ages 12 to 17 received treatment.
Oklahoma has the ninth worst mental health system for youth, based on prevalence and access to care and is dead last in providing mental health coverage to children. Sadly, the average delay between onset of symptoms and intervention is 8 to 10 years.
“Mental health is similar to a lot of other health conditions in the sense [that] there are some that could go away spontaneously, but most problems get worse if ignored,” said Dr. Naveena Boindala, child and adolescent psychiatrist for INTEGRIS Mental Health, Spencer. “The tricky part of mental health is that it affects the very core of who you are as a person if you are affected by it at an early age.”
Without early and effective identification and intervention, childhood mental health conditions can lead to failure in school, poor employment opportunities, substance abuse, poverty, homelessness, incarceration and suicide.
“The benefits of seeking help at an early stage are you can actually change the direction your child is headed and take action when you have the power to,” said Boindola.
 According to the National Alliance on Mental Illness, nationwide half of students age 14 or older with a mental health condition drop out of high school. That’s the highest dropout rate of any disability group. More than half of the adults in the country with a substance use disorder also have a mental health condition. Seventy percent of youth in the juvenile justice system have at least one mental health condition. More than one fourth of homeless adults staying in shelters live with a serious mental illness. As kids with serious untreated mental health condition grow to adulthood, they die on average 25 years earlier than their peers, often due to treatable medical conditions.
According to the National Alliance on Mental Illness, nationwide half of students age 14 or older with a mental health condition drop out of high school. That’s the highest dropout rate of any disability group. More than half of the adults in the country with a substance use disorder also have a mental health condition. Seventy percent of youth in the juvenile justice system have at least one mental health condition. More than one fourth of homeless adults staying in shelters live with a serious mental illness. As kids with serious untreated mental health condition grow to adulthood, they die on average 25 years earlier than their peers, often due to treatable medical conditions.
Perhaps most frightening, suicide is the second-leading cause of death in Oklahoma for youth ages 10 to 24, with one in 15 Oklahoma youth reporting attempted suicide. That’s as many as two students in an average middle school classroom. Nationally, 90 percent of youth who committed suicide had an underlying mental health condition.
For many, the words “mental health condition” connote violent behaviors, desire for attention, an inability to regulate emotions or mental weakness. The resulting stigma can be nearly impossible to live with. In actuality, mental health conditions are diseases that require treatment, just like diabetes or asthma.
“No more than a person with a physical illness is to blame for their problem, neither is the person to blame for their mental health disorder,” said Dr. Wana Ellison, chief operating officer-outpatient offices of Red Rock Behavioral Health Sciences.
Recognizing the Signs
According to the Centers for Disease Control, attention deficit/hyperactivity disorder is the most prevalent mental health diagnosis among children age 3 to 17 years, followed by behavioral or conduct problems, anxiety, depression and autism spectrum disorders. Dr. Lisa Marotta, an Edmond psychologist, most commonly sees children with anxiety disorders, including generalized anxiety disorder, obsessive compulsive disorder and phobias. She also treats children with attention-deficit hyperactivity disorder, depression and autism spectrum disorder.
“Most children who are referred for mental health services are experiencing a combination of mood and behavior symptoms,” said Marotta.
Every child goes through periods of worry, moodiness, trouble concentrating and the like, especially when faced with significant changes like moving, a new sibling, a divorce or the death of a loved one. It’s often difficult for parents to differentiate between developmentally-appropriate behaviors and cause for greater concern.
“Most of the time children are able to get back to their normal state a few days or weeks after the stressful event, in which case intervention may not be necessary,” said Boindola. “If behavior or mood changes persist or start to significantly cause your child distress in their academics, social activities or relationships, it could be time to intervene.”
Marotta says the key differences between a developmental fluctuation and symptoms of a mental health condition are how long the change lasts and how much it impacts the child’s social and academic life.
“Every child is going to have a no good, very bad day occasionally, but when bad days are more the norm, more support is indicated,” said Marotta. “Two weeks of consistently sad, anxious or angry mood is a long time for a child.”
Key indicators of a mental health condition don’t always look the same in children as they might in adults. Children may sleep significantly more or less, gain or lose weight, withdraw from friends and family, experience intense worry or fear, avoid places or activities they once enjoyed, or feel unmotivated. Anxious and depressed children don’t always seem overly nervous or sad. Instead, they may consistently be irritable or complain of physical maladies, like headaches or stomachaches.
Lori Wharton’s daughter complained often of physical aches and pains at age 12. On one occasion she was in so much pain that Wharton took her to the doctor, certain she had a broken arm. She didn’t.
“Children can become very irritable, complain a lot, say they’re bored or express a lot of negativity,” said Wharton.
When her daughter (who asked to remain unnamed) would say she hated her life, Wharton was quick to remind her of all their blessings. Now she realizes she was dismissing her daughter’s intense feelings.
“It’s the same thing as telling someone experiencing chest pain ‘oh you’re fine; your chest doesn’t hurt,’” said Wharton.
Wharton combatted her daughter’s boredom by seeking new activities she thought she’d enjoy, none of which struck a chord. Her daughter experienced separation anxiety, often worrying about her parents dying. Her symptoms escalated to two suicide attempts.
“I didn’t think it could happen to families like us,” said Wharton, who now educates parents about the signs of depressed and suicidal children and youth through Mental Health Association Oklahoma’s board of directors and suicide prevention program. “If I had had that training, I would have been comfortable enough to ask her if she was thinking of hurting herself. I could have prevented our daughter’s suicide attempts.”
Wharton describes her daughter, now in college, as successful, well-adjusted and extremely empathetic to her friends’ feelings. She’s an advocate for other youth getting mental health support. Though their journey has a positive ending, it was tumultuous. Finding the best combination of medications, the right therapist and the right therapy took nearly two years. As Wharton navigated Oklahoma’s mental health system, she often felt isolated and overwhelmed.
“No one talks about any of this,” said Wharton. “I didn’t have anyone say ‘this is okay; this is going to get better.’”
Fighting Back
When a child shows signs of a mental health condition, Wharton and experts alike urge parents to simply listen, without dismissing feelings.
“Put aside all of the judgment, opinions and your past experiences,” said Ellison. “Focus on what they are trying to communicate and really listen to the person in pain.”
Social rejection or pressure to perform academically or athletically can initiate or exacerbate mental health conditions. Wharton’s daughter was bullied and she says she made the mistake of comparing their childhoods.
“I got through being bullied and she will, too,” Wharton says of her initial reaction. “You have to recognize the difference between having a hard time and something chronically going on. Sometimes it’s hard when you’re living it every day.”
That’s why it’s critical to seek the help of experts. When symptoms arise, the first step for parents is to talk with the child’s pediatrician about their concerns and get a referral to a mental health specialist.
“It is important to choose the right therapist and doctor,” said Boindola. “Ask a lot of questions at your visit: ask about diagnosis, course of the disorder, treatment options and non-medication alternatives,” said Boindola.
Most mental health conditions are treated with a combination of therapy and medication, and parents should seek specific information about what type of therapy is recommended, potential side effects of any medication and whether the therapist or doctor has experience treating the child’s condition.
Mental Health Association Oklahoma’s Teen Screen program is another avenue for parents seeking an objective, professional assessment of their child’s mental health. The free youth wellness screening program identifies general health and mental health concerns in students in grades 6 through 12. The screenings are conducted individually by appointment and in some Oklahoma schools. If a screener identifies a mental health concern, parents are notified and supported in getting the child treatment.
Though it’s emotional for Wharton to look back on her daughter’s suicide attempts and subsequent family journey, she chooses to channel those emotions into helping others. She hopes that by sharing their experience she gives other families the freedom to break free of stigma and seek support.
“You’re going to feel guilt, but it’s a useless emotion,” said Wharton. “You love your kid and do the best that you can and look forward.”


